Starting in the 1970s, anthropometric measures have increasingly been used in the social sciences as indicators of social well-being. Since then, adult height has been considered an indicator of the general health status in life, of the relative risk of survival, and labor productivity (Fogel, 1986). In particular, Case and Paxson (2008) explain the positive correlation between adult height and labor productivity by showing that height is positively associated with cognitive ability. They show that both cognition and height are driven by early childhood investments and therefore cognitive achievements are correlated with height, and wages are affected by cognitive skills. Poor health can explain both low height and low labor productivity. This is more evident in developing countries where living conditions are poor. However, adult height is just the final result of a process of growth that involves many different mechanisms and variables, and most of the common evidence looks at adult height (Steckel, 2009). It is therefore necessary to investigate the factors driving height, since understanding the determinants of height is important in order to understand health (Deaton, 2007). The determinants of height can be divided into non-genetic factors, genetic factors and the age when height is measured. The principal non- genetic factor is net nutrition which is the difference between food intake and the losses to activities and to diseases (Eveleth and Tanner, 1991).
To study the determinants of height from birth to maturity I use in my last CSAE working paper the Cebu Longitudinal Health and Nutrition Survey (CLHNS), which is a rich longitudinal survey of a cohort of Filipino children followed from conception, in 1983-84, to 2005. The distribution of height by age and sex is shown in Figure 1.
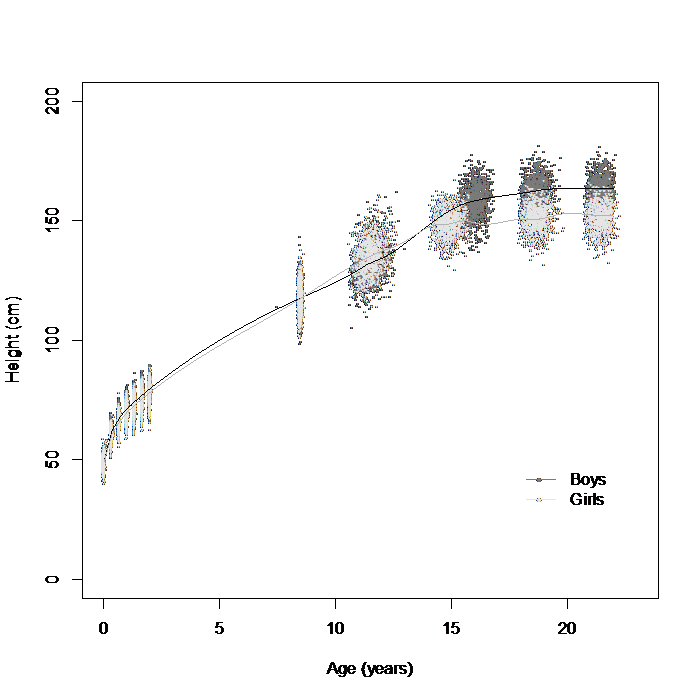 Figure 1: Height distribution by age and gender of the child. The dots correspond to the raw height measurements, while the lines correspond to spline interpolation of the mean height per gender and age of the child.
Figure 1: Height distribution by age and gender of the child. The dots correspond to the raw height measurements, while the lines correspond to spline interpolation of the mean height per gender and age of the child.
I build and estimate a height production function which depends on age, previous investments in the child, biological endowment and a shock. To study empirically the height production function, I assume (A) that the child’s biological endowment is determined at conception and is constant over time, and (B) that the height production function is linear in the inputs and in the unobserved endowment, and that the effects of the inputs depend on the child’s age. I can then specify a model where the current height is regressed on a function of age (linear and a quadratic age), current and past inputs (nutrition and diseases), a child’s fixed effect and a shock.
The nutrition inputs considered are the caloric intake and breast feeding. I distinguish between diseases experienced during infancy, pre-puberty and puberty because they are age-dependent and might have a different impact on a person’s growth, and moreover the data contain different measures of morbidity that differ between waves. In particular, I consider diarrhea episodes experienced during infancy, length of stay in the hospital during pre-puberty, and hospitalization during puberty (dummy if the child has been hospitalized).
In order to estimate this model, I consider a within-child fixed effects specification (FE) where I estimate the change in height between two consecutive measurements, remaining only with the contemporaneous inputs. However, contemporaneous inputs could respond to previous shocks causing endogeneity because correlated to unobserved parental preferences regarding their children’s nutrition and preventative care. I address endogeneity of both nutrition and diseases by using variation in village-level food prices, village and household characteristics, and climatic shocks as instrumental variables (IV) to estimate the production parameters via IVFE.
The IVFE results show that the diarrhea episodes experienced during infancy, and in particular in the second year of life, have the largest and negative effects on height. If experienced in the first year of life, an increase by one of the diarrhea episodes decreases the height of a boy by 1.376 cm, and the height of a girl by 2.113 cm. Experiencing an extra episode of diarrhea in the second year of life, reduces the height of a boy by 2.214 cm, and the height of a girl by 3.171 cm. Diseases experienced later in life and measured with time spent in the hospital or number of hospitalizations do not seem to affect height. Pre-puberty (age 8 and 11) is dominated by the effects of nutrition. The IVFE estimates show that if caloric intake increases by 100 kcal then height increases in 8 year old boys by 0.199 cm, in 11 year old boys by 0.246 cm, and in 11 year old girls by 0.200 cm. It might be that the pre-puberty years prepare the body for the final phase of growth, and that might explain the relevance of nutrition inputs at age 11 and also age 8 for boys.
Overall, these results show that growth in infancy and in the pre-puberty years turn out to be critical stages in the process of height formation. This is in line with the increasing literature on the long term effects of early life conditions (Almond and Currie, 2011) and with new studies that reveal the importance of later critical periods (van den Berg et al., 2014). Most importantly the paper shows that some critical periods are important because diseases experienced during infancy play a major role compared to nutritional intake. This might be important to design policy interventions that target individuals in these critical periods to improve their health and potentially their socio-economic outcomes later in life.
Elisabetta De Cao – Centre for Health Service Economics & Organisation, University of Oxford
New Radcliffe House (2nd floor), Walton Street, Oxford, United Kingdom (e-mail: elisabetta.decao@gmail.com; elisabetta.decao@phc.ox.ac.uk)
References
Almond, G. and J. Currie, 2011. Human capital development before age five. In O. Ashenfelter, R. Layard, and D. Card, editors, Handbook of Labor Economics, volume 4B, chapter 15, pages 1315–1486. Amsterdam, The Netherlands: North- Holland.
Case, A. and C. Paxson, 2008. Stature and status: Height, ability, and labor market outcomes. Journal of Political Economy, 116(3):499–532.
Deaton, A., 2007. Height, health, and development. Proceedings of the National Academy of Sciences, 104(33):13232–13237.
Eveleth, P. and J. M. Tanner, 1991. World-Wide Variation in Human Growth. Cambridge. Cambridge University Press, second edition.
Fogel, R., 1986. Physical growth as a measure of the economic well-being of popula- tions: The eighteenth and nineteenth centuries. In F. Falkner and J. M. Tanner, editors, Human Growth: A Comprehensive Treatise, volume 3, pages 263–281. New York: Plenum Press.
Steckel, R. H., 2009. Heights and human welfare: Recent developments and new directions. Explorations in Economic History, 46(1):1–23.
van den Berg, G. J., P. Lundborg, P. Nystedt, and D. O. Rooth, 2014. Critical periods during childhood and adolescence. Journal of the European Economic Association, 12(6):1521–1557.

Very informative article, i’m regular reader of your website.
I noticed that your website is outranked by many other websites
in google’s search results. You deserve to be in top ten. I know what can help you, search in google
for:
Omond’s tips outsource the work